












































Timing of Information-Seeking about Infant Vaccines
University of Colorado Anschutz Medical Campus (O'Leary, Dempsey); University of Colorado/Children's Hospital Colorado (O'Leary, Brewer, Pyrzanowski, Barnard, Sevick, Furniss, Dempsey)
Studies have shown that an increasing number of parents in the United States (US) are either refusing or delaying vaccines for their children. Although most parents identify their child's physician as their most trusted source of information, many parents, vaccine-hesitant or not, seek information about vaccines from other sources, particularly the internet, a medium prone to containing misinformation. The objectives of this study were to assess, among pregnant and recently delivered women, the timing of thinking about and seeking information about infant vaccines, and preferred modes of communication about infant vaccines.
From January to February 2014, the researchers administered an email survey to 230 eligible women who were patients at obstetrics/gynaecology (OB/GYN) practices (6 urban, 3 rural) in Colorado, US. Recall bias was reduced by asking the women to report their thoughts and actions over the previous 2 weeks, rather than in more distant retrospect. In addition, questions about vaccination were embedded into a larger survey, further reducing bias. Vaccine hesitancy was assessed with 2 questions from the Parent Attitudes About Childhood Vaccines (PACV) survey, a validated scale of vaccine hesitancy: "How hesitant about childhood vaccines do you consider yourself?" and "How concerned are you that one of the childhood vaccines might not be safe?"
Among respondents, 56% were pregnant and 44% had delivered. Overall, 2% (n=5) reported being "very hesitant" and 16% (n=37) reported being "somewhat hesitant" about vaccines, and 19% (n=44) reported being "somewhat concerned" and 8% (n = 18) reported being "very concerned" that at least 1 childhood vaccine might not be safe. Although 45% (n=103) of the study population considered themselves "not at all" vaccine-hesitant, only 26% (n=60) reported being "not at all" concerned about vaccine safety.
Ten percent of women reported seeking information about infant vaccines "often", 27% responded "sometimes", 24% responded "rarely", and 38% responded "not at all". Similar to the frequency of thinking about infant vaccines, women who had delivered reported seeking information about infant vaccines more often than those who were pregnant. This finding also was consistent in vaccine-hesitant participants, in whom "often" or "sometimes" seeking vaccine information was more common after delivery (19% and 44%, respectively) than while still pregnant (9% and 26%, respectively; P = not significant).
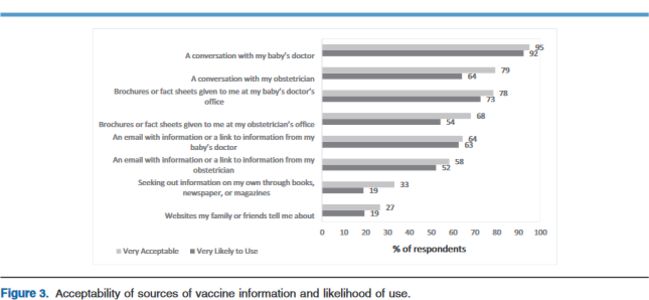
Most women preferred a conversation with their child's doctor compared with other sources of childhood vaccine information, with 95% of women reporting this as a "very acceptable" source of information, and 92% responding that this is a source they are "very likely" to use. Most women also were amenable to conversations and information about childhood vaccines from their obstetrician. More than one-half of women reported being likely to use web-based information provided by either their obstetrician or their child's doctor. Other sources of information, such as books, newspapers, or magazines and websites suggested by family and friends, were favoured less often. There were no significant differences in these responses between pregnant and recently delivered women or between hesitant and nonhesitant respondents.
This study suggests that along with offering information about vaccination during pregnancy, providing accurate information shortly after delivery may reach the most women and have the most impact. This time window should be evaluated further as an opportunity for providing education to new parents. Even in mothers who are not vaccine hesitant, this period also seems crucial for providing accurate vaccine-related information. Although the baby's doctor is the most preferred source of childhood vaccine information, obstetric providers might consider providing such information in their offices (for example, at the postpartum visit, which would correspond with this time frame). Web-based information sent from the provider's office appears to be acceptable to most women and thus could be considered in future interventions. In addition, investigators in this field may wish to consider replicating this work in more diverse populations with a larger sample size.
The Journal of Pediatrics 2018;203:125-30. https://doi.org/10.1016/j.jpeds.2018.07.046
- Log in to post comments